Slide 11 of 47
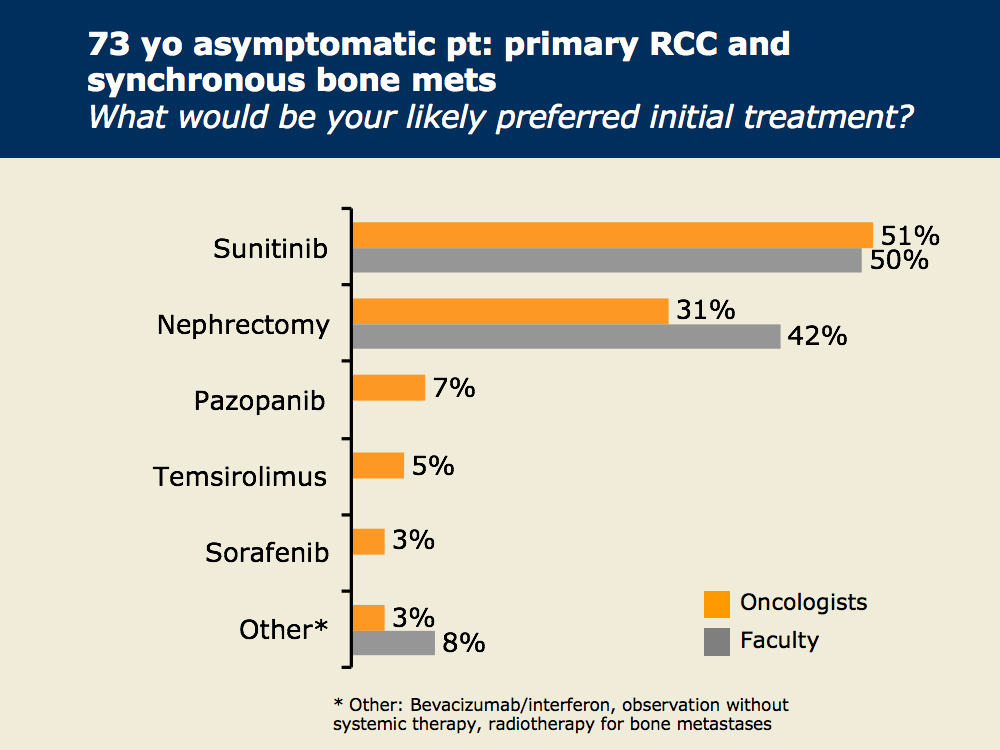
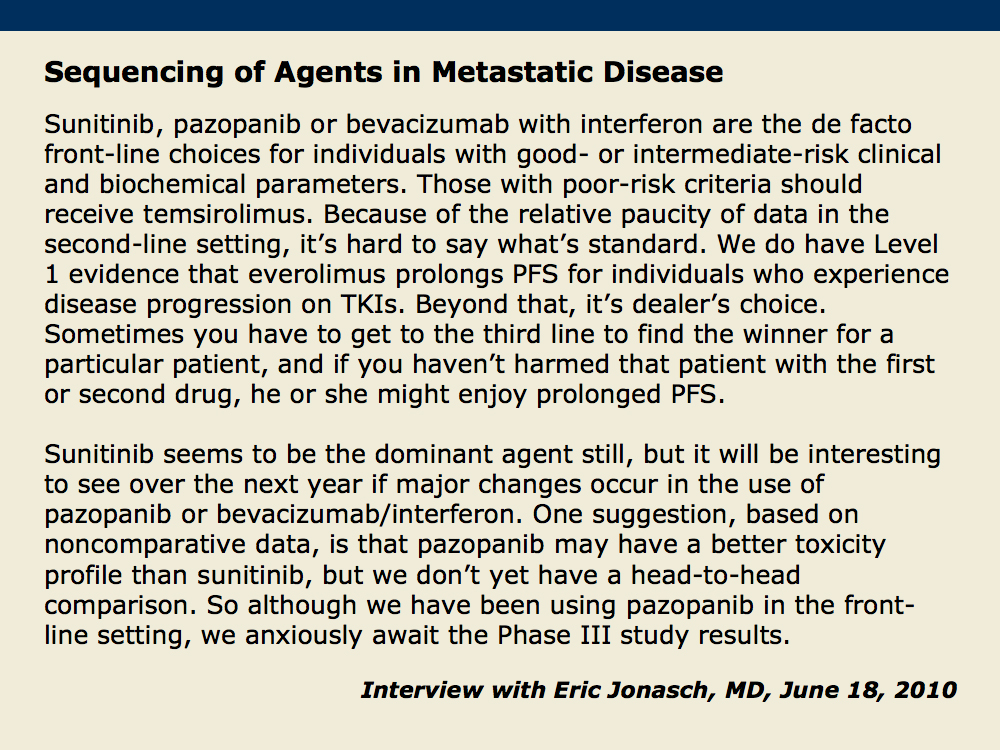
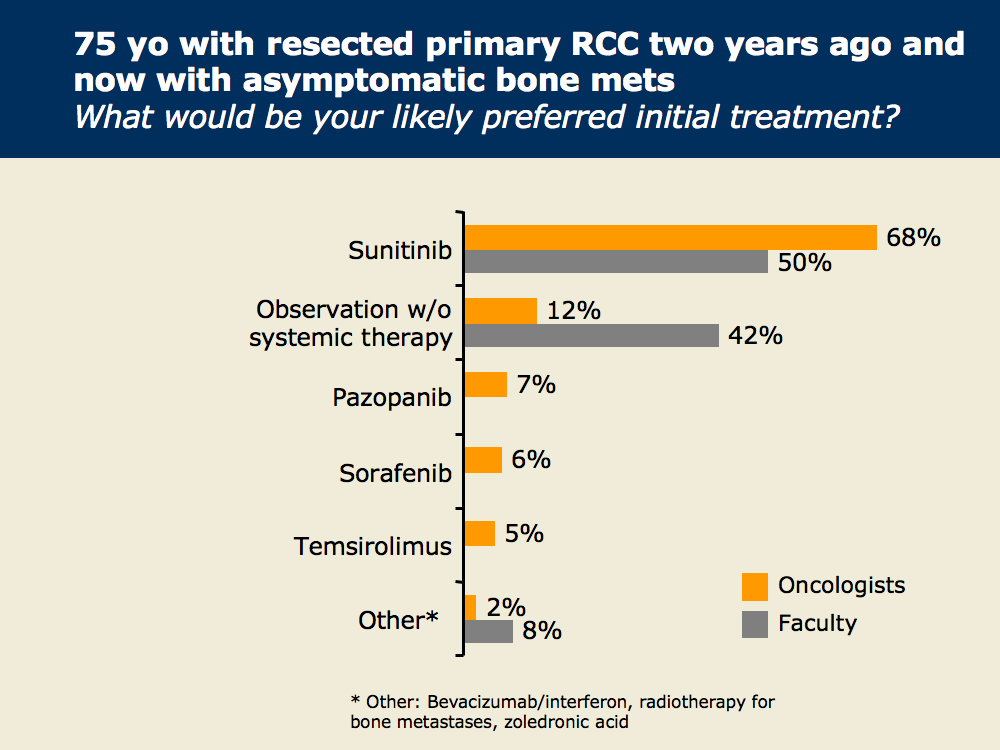
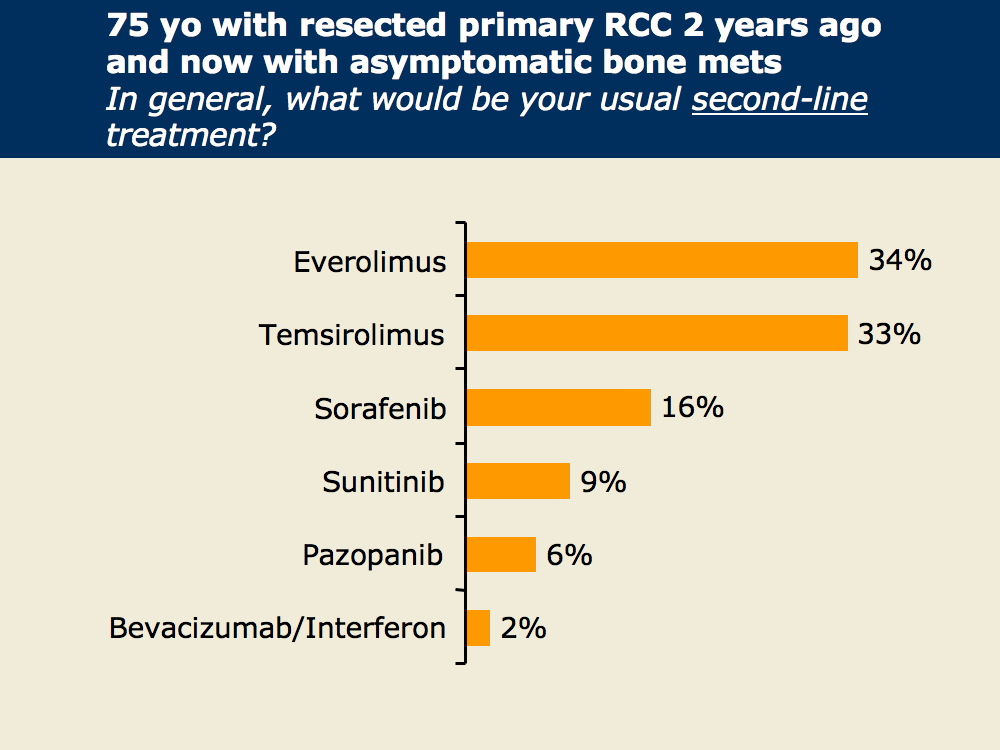
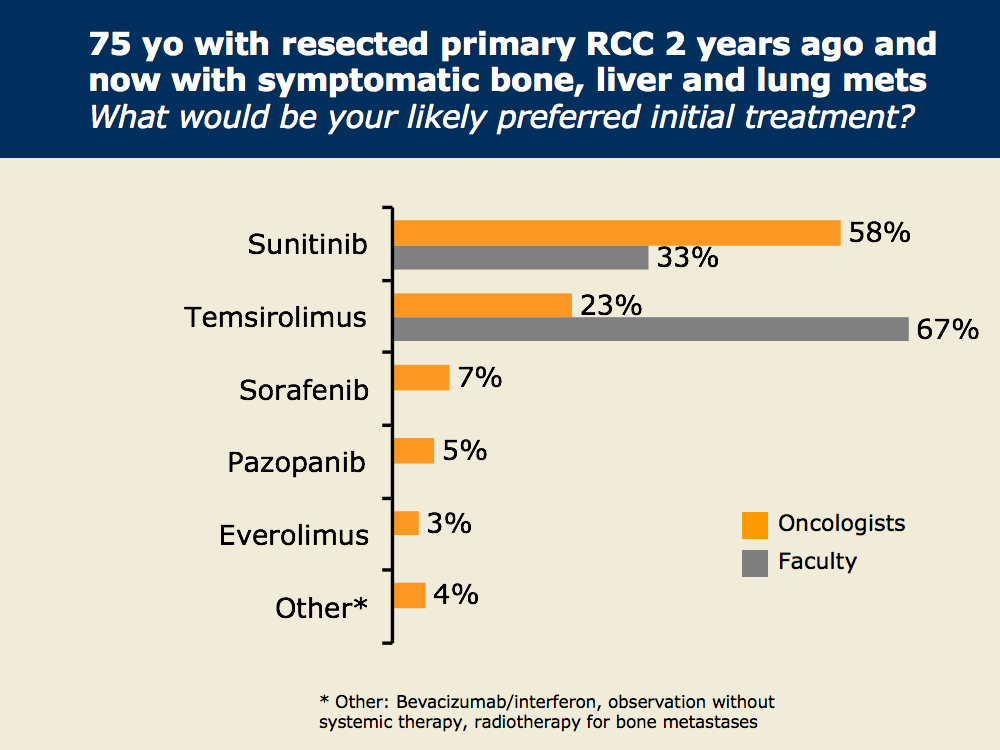
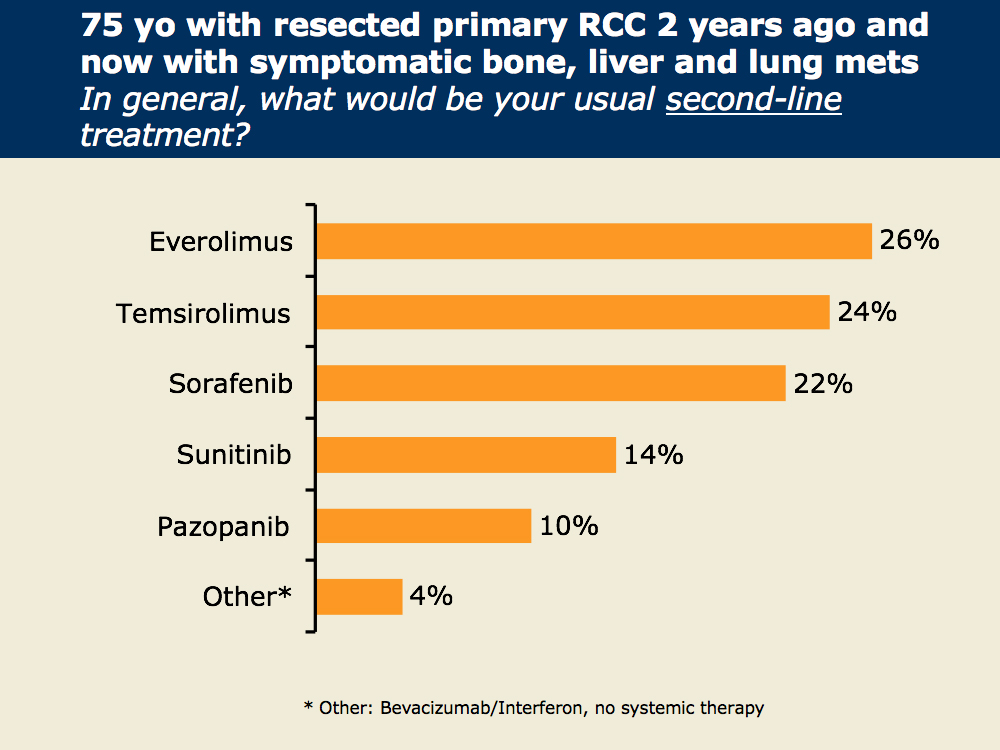
Dr Jonasch notes that in the most common scenario, in which patients do not have emergent clinical and biochemical findings, the evidence-based first-line options in his mind are sunitinib, pazopanib and bevacizumab/interferon. For first-line treatment of patients with poor-risk disease, temsirolimus has been studied the most extensively and is standard, and while there is no standard second-line treatment after TKIs, everolimus has clinical trial data supporting its use for these patients.